What’s a lipidologist? Well, immediately we can see that the term’s Latin roots indicate that a lipidologist is someone who studies lipids. Ah, lipids: the dreaded cholesterol, et al. That seemed simple enough. A friend told me that a lipidologist practiced in Santa Fe, the only one in the whole state of New Mexico.
Okay, it’s a small state, population around 2 million, about half that of the city of Los Angeles, California. Only about 400 lipidologists work in the entire U.S. Why are they so rare? After all, blood lipids are a big deal these days. Interestingly, there is very little information in Wikipedia’s entry on Lipidology.
Despite its simple bad reputation, cholesterol is far more complicated than a mere matter of suppressing “bad” cholesterol and supporting “good” cholesterol in the bloodstream. The drug companies have worked hard to popularize the idea that cholesterol is “bad.” We produce cholesterol in the liver and we ingest it in the food we eat.
So, why do they cast cholesterol in such a bad light? Think drug company profits. I won’t get into the complex disputes over the efficacy and dangers of statin drugs in attempting to control cholesterol in the bloodstream. Or the role statins play in minimizing the risk of plaque building up in the coronary arteries. Suffice it to say, it is not all science.
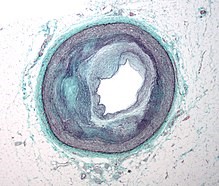 Picture to the left is a Micrograph of an artery that supplies the heart showing significant atherosclerosis and marked luminal narrowing. Tissue has been stained using Masson’s trichrome. As Dr. M. explained, old plaque is scar tissue, and may not necessarily cause such blockage. High performance on a stress test indicates no blockage of cornonary arteries. Unlike new plaque, old plaque does not flake off, risking heart attack or stroke, unlike new plaque. However, both contain calcium, so measures of plaque do not distinguish between the two. So, you can have a very high score for plaque, pass the stress test indicating no blockage, and have low risk. Yet most cardiologists don’t make such distinctions; they just prescribe statins. If my arteries looked like the one in the picture here, I could not have passed the stress test with ease, as I did.
Picture to the left is a Micrograph of an artery that supplies the heart showing significant atherosclerosis and marked luminal narrowing. Tissue has been stained using Masson’s trichrome. As Dr. M. explained, old plaque is scar tissue, and may not necessarily cause such blockage. High performance on a stress test indicates no blockage of cornonary arteries. Unlike new plaque, old plaque does not flake off, risking heart attack or stroke, unlike new plaque. However, both contain calcium, so measures of plaque do not distinguish between the two. So, you can have a very high score for plaque, pass the stress test indicating no blockage, and have low risk. Yet most cardiologists don’t make such distinctions; they just prescribe statins. If my arteries looked like the one in the picture here, I could not have passed the stress test with ease, as I did.
Dr. M. occupies a modest office in the local cluster of medical practices near the only hospital in Santa Fe. When I went to see him, he seemed in no hurry and spent an hour and a half with me. We had a very informative (for me) conversation about heart disease, medical practice, and the flaws of scientific practice in medicine in the U.S., where so many decisions are controlled by the insurance companies and where medical practices are dominated by the drug companies – otherwise known as “Big Pharma.”
When Dr. M. described the complex of bio-chemical, genetic, environmental, and behavioral elements that are involved with the multiple variable factors in the way cholesterol acts, I was impressed. No cardiologist had ever mentioned any of this stuff to me. It had always been a simple, “if your LDL is too high, take [the latest statin drug].” End of story.
The practice of medicine is too often a high-volume assembly-line operation that executes the “standard of care” in conformity to the specifications of Big Pharma and the medical insurance industry. Dr. M. does not play that game. He and a few other practicing medical scientists carefully measure the complex of interacting factors that may be at play in each individual and adjust treatments based on re-testing of bio-chemical and genetic factors and patient characteristics. Such doctors epitomize the scientific practice of medicine.
Medicine, it seems to me, should involve the scientific study and practice of treatments, traditional as well as modern, of potential benefit to patients. It requires carefully testing the efficacy of each treatment for a particular problem and adjusting treatment to the conditions of the individual patient. It is far more labor intensive than simple prescribing pills in accordance with the “standard of care.” I know only one lipidologist, but if he is representative of others in the specialty, then lipidology represents the best practices in medicine.
Lipidology is to the “standard of care” in cardiology as prostate oncology is to the “standard of care” among urologists, who are surgeons.
